Welcome to Well Oiled Life with Tammy
Sensory Resets: Tune Into Your Body's Natural Rejuvenation

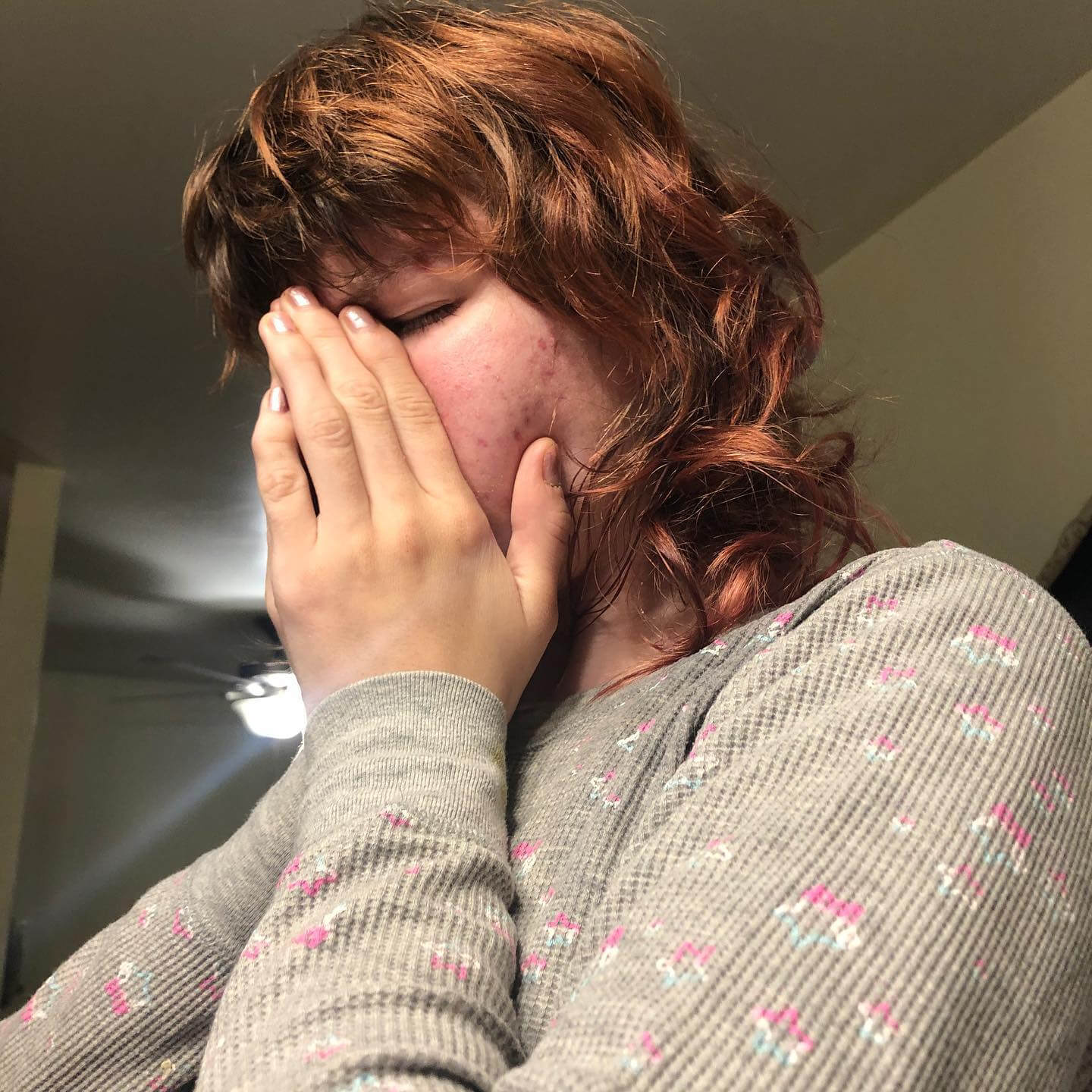
I see you ... because I have been there too!
You’re a woman who gives everything for your family and your work. You’re self-employed because you desire your freedom to be home more, and yet somehow, you feel even more stretched thin—caught between responsibility and your deep desire for spiritual connection, inner peace, balance, and time for yourself.
Me too.
I know what it’s like to carry the weight of it all, to long for your sense of ease in your home, your body, and your mind.
That’s why I’ve created space where you can let go of your stress, reset your energy, and realign with what truly matters.
That’s why I’ve created space where you can let go of your stress, reset your energy, and realign with what truly matters.
If you’re ready to feel lighter, calmer, and more in tune with yourself—I’m here to help.
✨ Explore how vibrational wellness, essential oils, and holistic healing can bring you back to center.
Your path to spiritual renewal and wholeness begins by clicking below and scheduling time for you.
Schedule My Wellness Session Now!
Schedule My Wellness Session Now!
Sample Service Options







about Your experience
Discover your inviting space designed for relaxation, rejuvenation, and holistic wellness.
Feel welcomed, heard, at ease and secure as you receive your personalized wellness session.
Feel welcomed, heard, at ease and secure as you receive your personalized wellness session.
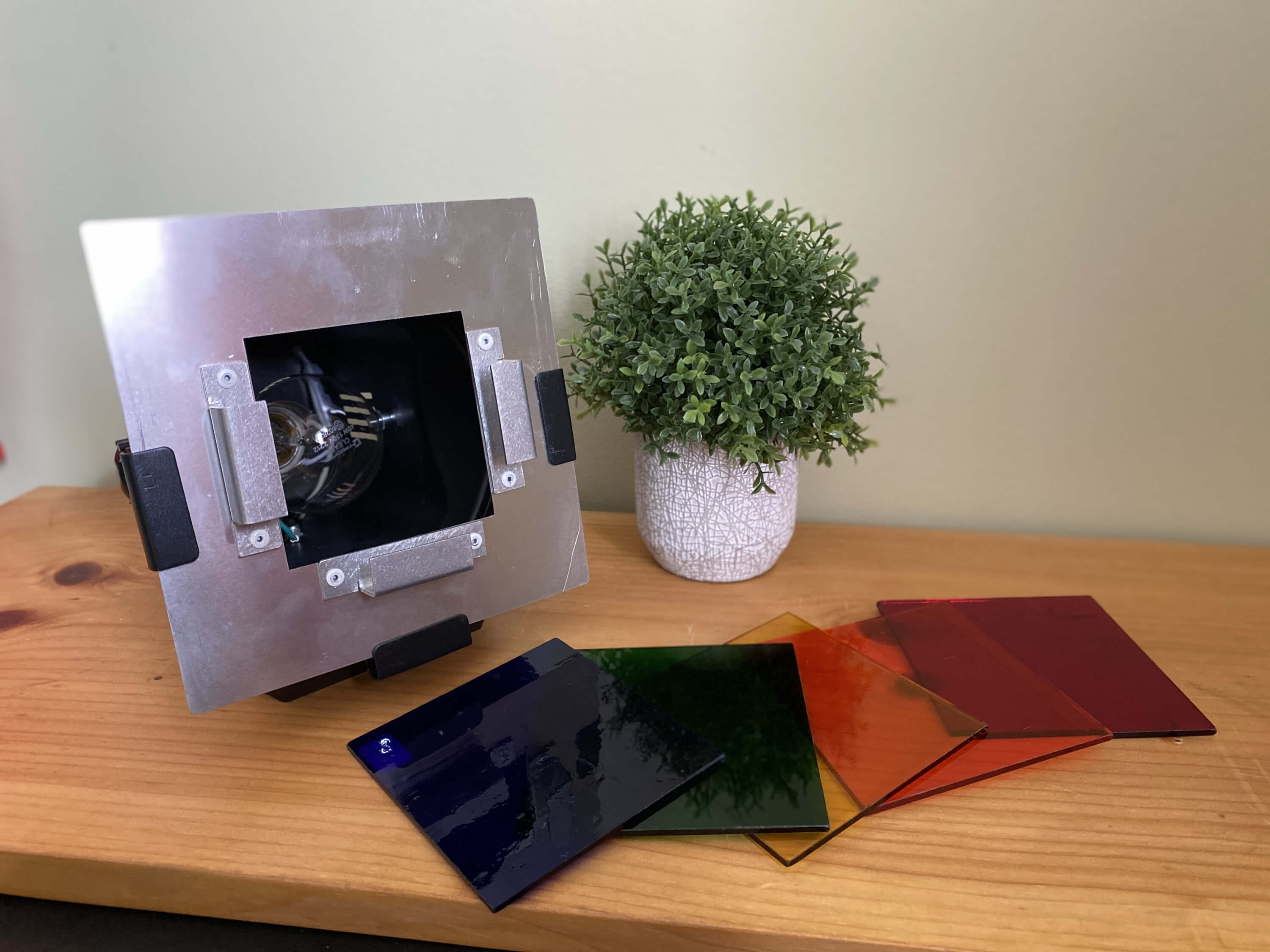
Through specialized, unique, cutting edge, services, including tuning forks, vita flex, color light, crystals. conscious language and pure essential oils, receive your restorative, balancing, rejuvenating, personalized experience, as you embrace your sense of nourished self care.
Simply enjoy, relax and let go with ease, as you renew your spiritual connection!
Simply enjoy, relax and let go with ease, as you renew your spiritual connection!
.

Ready to Begin Your Healing Journey?
YOUR EXPERIENCE, UNIQUELY YOURS

Intuitively led wellness sessions, are personalized for your unique custom experience.
During your wellness session a variety of services may be provided for your restored sense of well being.
Your session may include improving your vitality, some refreshing light on your situations, improved inner harmony, sensory activation and much needed relaxation.
You will leave feeling recharged, rejuvenated, and energized.
Ready for your session? Schedule below!
You will leave feeling recharged, rejuvenated, and energized.
Ready for your session? Schedule below!
Holistic Wisdom for Your Balanced Life
Stay Connected with Tammy
Subscribe to my newsletter here for wellness tips, spiritual guidance, recipes, upcoming event and special offers
To subscribe, click here





Copyright 2025 Tammy Hawskworth
Disclaimer Notice:
I am not a medical professional, therapist or counselor, as a result, I do not treat, diagnose, or prescribe. Please seek out your medical professional for such services.
Raindrop, and Aroma Freedom Technique, Tuning forks, color lights, essential oils and Sacred Body Language Translations are non-medical and are not designed to replace, treat or diagnose any medical condition or current treatments. Please continue with or seek our medical professionals are required.
I am not a medical professional, therapist or counselor, as a result, I do not treat, diagnose, or prescribe. Please seek out your medical professional for such services.
Raindrop, and Aroma Freedom Technique, Tuning forks, color lights, essential oils and Sacred Body Language Translations are non-medical and are not designed to replace, treat or diagnose any medical condition or current treatments. Please continue with or seek our medical professionals are required.
The AFT process is also not psychotherapy and it not intended to replace any such treatments. The processes can bring up past memories and traumas, however the sharing of those situations and their details are not required for successful sessions. The process is based on neuroscience, the powerful affects and response to our sense of smell and the olfactory systems' nature and unfiltered function and ability to process emotions and memories, and was created by Dr. Benjamin Perkus, a clinical psychologist.. Each practitioner may add in their own personal style for the process.